As complexities in billing and coding pain management are increasing each year, it is important for practices to focus more on documentation as well as carefully handle pain management billing and coding. A reliable pain management medical billing company can support medical practices to efficiently manage their revenue cycle, while providers and staff can focus on patient care. For any medical specialty, solid coding and billing practices are crucial to receive accurate and timely reimbursement, prevent claim denials and audits, and maintain financial well-being.
It is critical for pain medicine providers to ensure that injections like facet joint injections and nerve blocks are accurately documented. Each patient visit has to be recorded in the original operative note or an addendum. Any missed information can delay the processing of the claims, resulting in denied or delayed reimbursement.
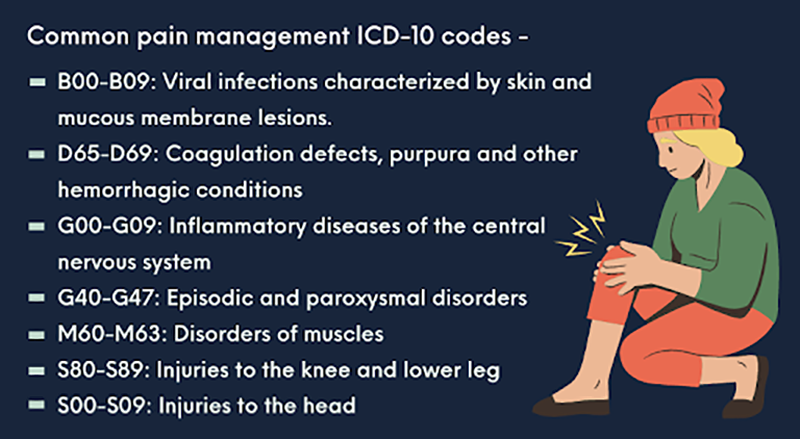
Pain Management Coding – Best Practices
Provide detailed diagnosis description
It is crucial to –
- include the cause, the site and laterality of the pain
- include a qualifier as well as specific details about the pain
Appropriate documentation of injections administered
Accurately document –
- details of the epidural injections
- various routes of administration for injections and the final position of the needle used
- fluoroscopically-guided interventions
- the diagnosis notes that support the procedure
- details of the specific medicine administered as injection
- trigger point injection to treat various muscle groups
Know the modifiers used in pain management
Some modifiers commonly used in pain management are –
- -LT: anatomically left-RT, anatomically right
- -50: bilateral (use them while coding bilateral procedures)
- -59: notes that a service or procedure is independent and separate from other services that were performed on that same day
- -52: incomplete procedure, stopping part of the procedure due to reasons other than patient well-being
- -53: incomplete procedure, the physician chooses to end a procedure for the patient’s well-being
Accurate reporting of codes
Remember that the codes change every year and it is essential to stay updated on these changes. Also, any missed or inaccurate recording of modifiers can result in claim denials. Stay up to date with billing guidelines and payer policies to ensure maximum reimbursement. Outsourcing medical billing tasks can help medical practitioners to focus on patients, instead of back-office tasks.

More from This Author