
Cataract operations account for a large volume of the claims in ophthalmology practices. This quick, painless surgery has improved quality of life for millions of Americans. About 2 million cataract removal surgeries are performed each year, according to statistics from the American Academy of Ophthalmology (AAO). Coding cataract surgery accurately is crucial for providing consistent patient care and maintaining the financial sustainability of an eye care facility. Partnering with a medical coding company that has a deep understanding of ophthalmology coding and billing can help ambulatory surgical centers (ASCs) to avoid denials and maximize reimbursement for cataract procedures.

Ready to Enhance Your Practice’s Financial Health?
Ask for our specialized Ophthalmology medical billing services!
Know the Codes
Knowledge about the coding and general billing requirements for cataract procedures is crucial for ambulatory surgical centers (ASCs) to prevent denials and ensure optimal reimbursement.
CPT Codes
66830 Removal of secondary membranous cataract (opacified posterior lens capsule and/or anterior hyaloid) with corneo-scleral section, with or without iridectomy (iridocapsulotomy, iridocapsulectomy)
66840 Removal of lens material; aspiration technique, 1 or more stages
66850 Removal of lens material; phacofragmentation technique (mechanical or ultrasonic) (eg, phacoemulsification), with aspiration
66852 Removal of lens material; pars plana approach, with or without vitrectomy
66920 Removal of lens material; intracapsular
66940 Removal of lens material; extracapsular (other than 66840, 66850, 66852)
66982 Extracapsular cataract removal with insertion of intraocular lens prosthesis (1-stage procedure), manual or mechanical technique (eg, irrigation and aspiration or phacoemulsification), complex, requiring devices or techniques not generally used in routine cataract surgery (eg, iris expansion device, suture support for intraocular lens, or primary posterior capsulorrhexis) or performed on patients in the amblyogenic developmental stage; without endoscopic cyclophotocoagulation
66983 Intracapsular cataract extraction with insertion of intraocular lens prosthesis (1 stage procedure)
66984 Extracapsular cataract removal with insertion of intraocular lens prosthesis (1 stage procedure), manual or mechanical technique (eg, irrigation and aspiration or phacoemulsification); without endoscopic cyclophotocoagulation
66987 Extracapsular cataract removal with insertion of intraocular lens prosthesis (1-stage procedure), manual or mechanical technique (eg, irrigation and aspiration or phacoemulsification), complex, requiring devices or techniques not generally used in routine cataract surgery (eg, iris expansion device, suture support for intraocular lens, or primary posterior capsulorrhexis) or performed on patients in the amblyogenic developmental stage; with endoscopic cyclophotocoagulation
66988 Extracapsular cataract removal with insertion of intraocular lens prosthesis (1 stage procedure), manual or mechanical technique (eg, irrigation and aspiration or phacoemulsification); with endoscopic cyclophotocoagulation
ICD-10-CM Codes
Under ICD-10 there are more than 100 codes to report diagnosis of cataracts. Some codes indicate laterality, with 1 (right eye), 2 (for left eye) and 3for both eyes. This number is reported as the sixth character for most codes that require laterality, (e.g., H20.21 Lens-induced iridocyclitis, right eye), but there are some codes where it appears as the fifth character (H26.33 Drug-induced cataract, bilateral). Other codes do not indicate laterality.
In ICD-10, cataract codes appear in the following chapters (source – www.aao.org/eyenet/article):
- Chapter 4 Endocrine, nutritional and metabolic diseases – Example: E10.36 Type 1 diabetes with diabetic cataract, E11.36 Type 2 diabetes with diabetic cataract, E20.9 Hypoparathyroidism, unspecified, E46 Unspecified protein-calorie malnutrition, E34.9 Endocrine disease, unspecified, E74.21 Galactosemia, and E88.9 Metabolic disorder, unspecified.
- Chapter 6 Diseases of the nervous system– Example: G71.19 Other specified myotonic disorders
- Chapter 7 Eye and ocular adnexa– Disorders of lens section (H25H28) for the most-used diagnoses
- Chapter 17 Congenital malformations, deformations, and chromosomal abnormalities– Example: Q12.0- represents anterior and posterior axial embryonal, pyramidal, blue, central, cerulean, congenital, coralliform, coronary, and crystalline cataracts.
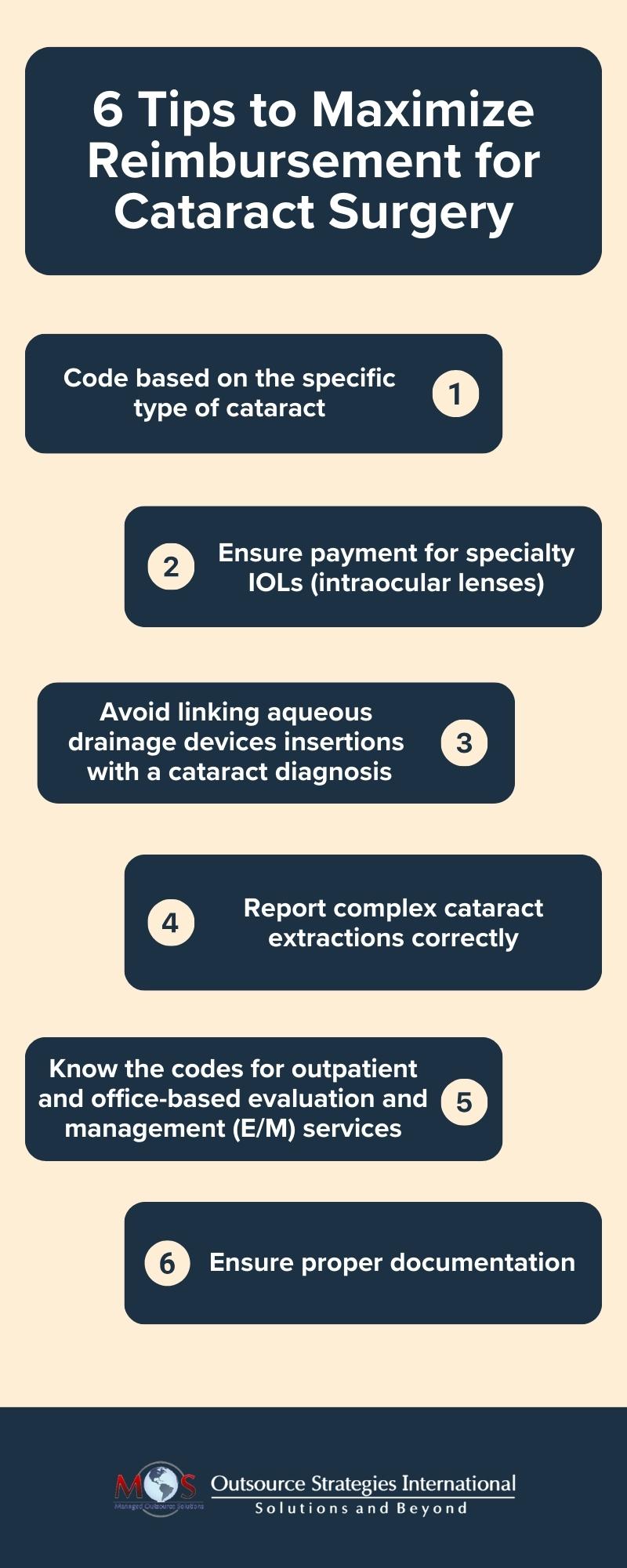
Coding Cataract Surgery – Expert Tips to Follow
- Code based on the specific type of cataract: Cataracts can be age-related, senile, diabetic, etc. The code assigned should be based on the cataract type as indicated in the physician’s documentation. ASCs should communicate with the physician to ascertain the specific type of cataract if it is not mentioned in the documentation. Do not bill for removing more than 1 cataract from the same eye. The AAO reports that one error that practices make which attracts audits is submitting the wrong CPT modifier or ICD-10 code when billing for a second cataract surgery.
- Ensure payment for specialty IOLs: Not collecting money for specialty IOLs will leave money on the table. Medicare pays for several specialty lenses from various manufacturers. ASCs should verify with the carrier whether there is an allowance for the lens and if it is not, they can collect the payment for the lens from the patient, preferably prior to the procedure. Patients should be informed about their potential financial responsibility for their lens prior to scheduling their procedure.
- Avoid linking aqueous drainage devices insertions with a cataract diagnosis: There is no medical necessity for aqueous drainage devices such as an iStent or CyPass for cataracts. So linking these devices to a cataract diagnosis can lead to claims denial. The devices are specific to the treatment of glaucoma and should be captured separately.
- Know the codes for outpatient and office-based evaluation and management (E/M) services: Ophthalmic exams are typically coded based on the number and severity of problems (High, Moderate, Low, Minimal), the extent of data reviewed (Extensive, Moderate, Limited, Minimal/None) and the level of management (High, Moderate, Low, Minimal).In 2021, changes were made to the method of selecting codes for outpatient and office-based evaluation and management (E/M) services. The focus shifted from documenting history and exam elements to medical decision making (most visits) or time (rarely).
Know what a Complex Cataract Extraction Means
A Beckers ASC Review report cautions that providers should know when CPT code 66982, which defines “complex” cataract extraction, can be reported. Understanding the guidelines for coding cataract surgery is especially important as this is an area under scrutiny by the Office of Inspector General (OIG).
- The AAO’sreply a question in March 2018 clarifies this matter. The question was: “The physician removed a mature pediatric cataract, which required the use of trypan blue. The surgery involved an anterior approach using the vitrector, rather than pars plana capsulotomy. She did not insert an IOL as it was not indicated. What is the best CPT code?”
- The AAO states that CPT code 66982 is not appropriate in this case because no lens was implanted, and recommends using code 66850, 66920 or 66940 (based on the operative note).
A www.eyeworld.org article lists some of the surgical complications that would not qualify as complex cataract extraction as: iris prolapse, vitreous loss, choroidal hemorrhages, and dropped nuclei.
According to www.medicarepaymentandreimbursement.com, indications for the use of code 66982 include: pediatric cataract surgery, extraordinary work that may occur when there is extreme postoperative inflammation and pain, mature cataract requiring dye for visualization of capsulorrhexis, and pre-existing zonular weakness requiring use of capsular tension rings or segments or intraocular suturing of the intraocular lens.
When submitting CPT code 66982, an AAO article reminds coders that local coverage determinations (LCDs) require more than the traditional cataract diagnosis codes. Examples include:
- H21.221 – H21.222 Degeneration of ciliary body
- H21.261 – H21.262 – H21.262 Iris atrophy (essential) (progressive)
- H21.561 – H21.562 Pupillary abnormality
- H21.81 Floppy iris syndrome
- H21.89 Other specified disorders of iris and ciliary body
- H21.9 Unspecified disorder of iris and ciliary body
- H22 Disorders of iris and ciliary body in diseases classified elsewhere
- H57.00 Unspecified anomaly of pupillary function
- H57.01 Argyll Robertson pupil, atypical
- H57.02 Anisocoria
- H57.03 Miosis
ASCs should review the operative report to determine which CPT and ICD-10 codes are most appropriate to report on the claim.
-
Ensure Proper Documentation
Make sure your documentation meets requirements. Here are some tips for accurate documentation from the AAO:
-
- Know local Medicare rules: Medicare Administrative Contractors (MACs) have LCDs that outline specific documentation requirements for the office visit that demonstrates the need for surgery (see: (https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleid=57195).
- Payer rules differ and may change: Check individual payer websites to understand their policy on the need for cataract surgery along with any preauthorization requirements. Additionally, as rules may change, follow the documentation requirements listed in the policy that was applicable at the time of surgery. Also VA requirements, if any, vary by payer.
- Examine if your previous documentation aligns with what you’ve submitted. If you have reservations about the accuracy of your documentation, consider conducting a self-audit of the data submitted over the last 12 months. Any errors can be rectified through a phone review.
Experienced coders in companies providing ophthalmology medical billing services are well-versed in the CPT and ICD-10 codes for this specialty. They will communicate with providers to get all the information necessary for coding cataract surgery procedures correctly. The services of expert coders and billing specialists can go a long way in maximizing ophthalmologists’ reimbursement.

More from This Author


